From Empirical to Evidence-Based: Accelerating Sepsis Decisions & Strengthening Infection Control
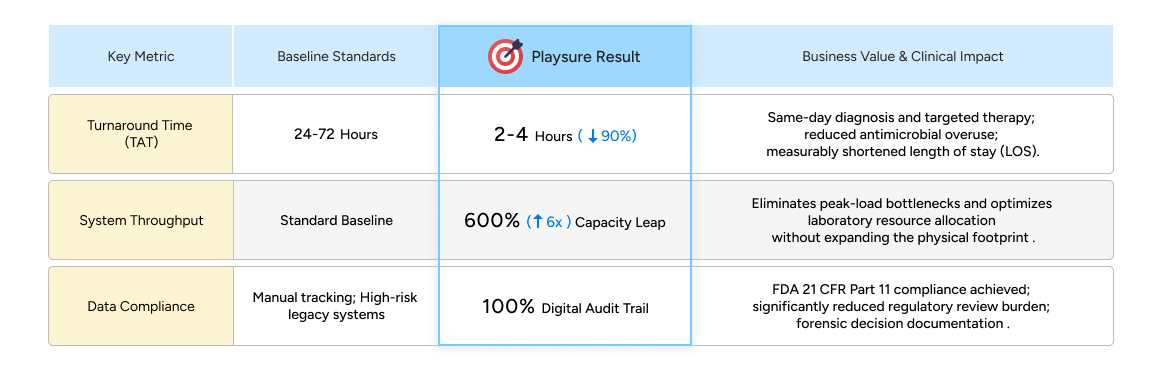
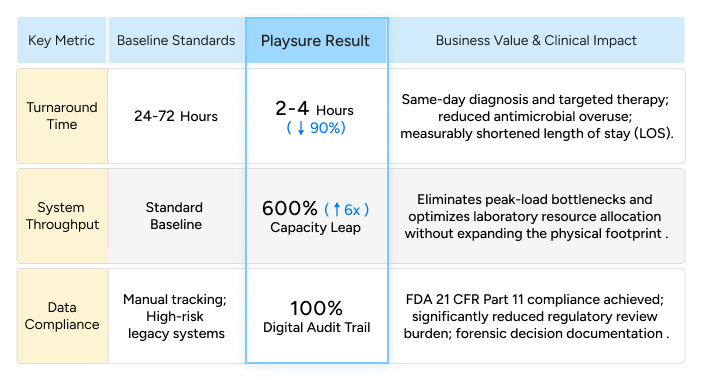
Precision medicine is the shared ambition of global healthcare. Yet, while therapeutics evolve rapidly, clinical diagnostics remain structurally disconnected due to biological and operational constraints. In sepsis and critical infection care, traditional AST (Antimicrobial Susceptibility Testing) still requires 24–72 hours—lagging significantly behind disease progression.
This prolonged "Diagnostic Blind Spot" forces clinicians to rely on Empirical Therapy during the golden window of survival. This systemic failure not only misallocates medical resources but also fuels the structural root of the global Antimicrobial Resistance (AMR) crisis, through prolonged empirical therapy and delayed treatment optimization.
To bridge this gap, Playsure, in strategic collaboration with National Cheng Kung University (NCKU) and Chi Mei Medical Center, acts as a catalyst for "Translational Engineering," advancing engineering approaches that connect research-grade precision with clinical application.
We go beyond hardware integration, focusing on translating academic innovation into system-level capabilities aligned with clinical workflows. By integrating advanced optical detection with algorithmic interpretation, we compress the AST cycle from 24–72 hours to just 2–4 hours—a 90% reduction that transforms clinical response. This eliminates the diagnostic vacuum, driving a paradigm shift from empirical guesswork to evidence-based precision within the same clinical shift.
#PrecisionMedicine
#AlgorithmicEngineering
#SystemArchitectureDesign
#RapidASTTesting
#RapidSepsisDiagnostics
#AntimicrobialStewardshipProgram